Hexie Quilting and a Puzzle
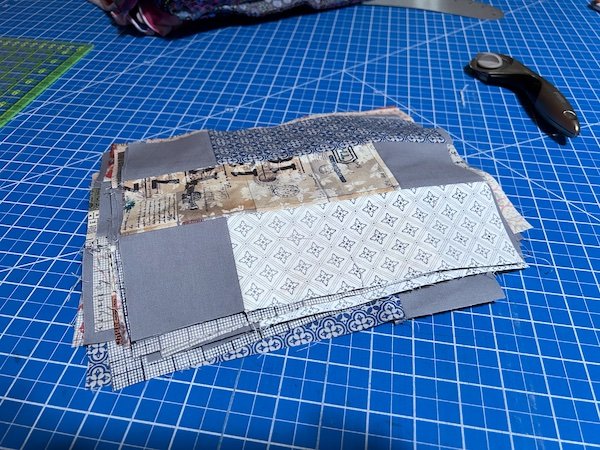
I spent yesterday making quilt backings. I couldn’t find any 108" wide fabrics that I liked at the quilt store, so I bought 44" wide yardage and pieced the backings. Then I basted them to the tops and batting. After lunch, I worked on quilting the EPP hexie wallhanging:

I’m stitching in the ditch around all the units. I’ll do something fun in the border. I’m just happy to be moving some of these projects through the pipeline.
Anna at Noodlehead released a new pattern, the Trail Tote:

I bought the pattern (of course), although I probably won’t make it immediately. I do love the piping detail. I carry a ton of stuff around with me—if we’re ever shopping together and you need a tape measure, I have one—so I would make the larger version. I think it would be great in a waxed canvas. I might order some of the waxed canvas that Sailrite sells just to see how it compares to the AL Frances canvas and the Klum House canvas.
So many things to make.
*******
I don’t talk about medical stuff very often here on the blog, because I am not a doctor and I don’t give medical advice, but I am living a medical puzzle and one of the pieces dropped into place this week. I am sharing in case it helps anyone else.
I am homozygous for the C677T mutation in the MTHFR gene. That means I got one copy from each of my parents. Maybe you’ve heard of MTHFR, maybe not. It has become more notorious thanks to DNA testing. (There is also a mutation known as A1298C, which I do not have.) The MTHFR gene codes for methylenetetrahydrofolate reductase, an enzyme involved in one of the metabolic pathways in our bodies. Because I am homozygous for that mutation, I have about 75% less methylenetetrahydrofolate reductase. The lack of that enzyme can lead to a laundry list of problems, and the fact that I got one copy of that gene from each of my parents means that it is running rampant on both sides of my family. We’ve done enough DNA testing that I know who has it and it what form.
Our first baby was born without a brain, a birth defect which falls under the category of neural tube defects and is directly attributable to that MTHFR mutation. It’s why pregnant women are now told to take folic acid. In my case, I don’t metabolize folate properly. You might think I could fix that by taking a folic acid supplement, but it’s more complicated than that. The folic acid that is available now is synthetic, and it actually causes more problems for people with MTHFR than it solves. A lot of doctors recommend methylfolate as an alternative, but I can’t take that, either, because it causes violent mood swings. I can tolerate folinic acid, which is a precursor to methylfolate, so I take that.
My mother has a B12 deficiency, also known as pernicious anemia. For most of her life, doctors told her to take more iron. 🙄 Pernicious anemia cannot be fixed by taking more iron. She requires B12 supplementation. That’s another manifestation of the MTHFR mutation.
That mutation can also cause elevated homocysteine which, in turn, leads to inflammation in the blood vessels. Blood clots, strokes, and heart attacks feature prominently in our medical history on both sides.
I want my girls to be armed with as much knowledge about this and how it affects them as possible, so I’ve done a ton of research. Thankfully, I have a naturopath as my primary care doctor who is also fairly knowledgeable about MTHFR. Most conventional doctors don’t have a clue.
I happened to be surfing Pinterest the other night when I ran across an article entitled, “Your ‘MTHFR’ is Just a Riboflavin Deficiency.” That led me to Chris Masterjohn, who has a PhD in Nutritional Sciences and a Substack account where he writes about this stuff. (The Substack account has a free version and a subscription version.) He argues that because the MTHFR mutations are so common—something like 75% of the population has a version of them—they’ve only become a problem for some people because the quality of our diets have deteriorated so much. I do know that I’d be happy to live on a diet of beans, rice, and leafy greens, all of which happen to be foods high in folate. My body knows what it needs.
Every so often, I get cracking and redness around my mouth. It’s more than just chapped lips. The dentist also told me in December that my tongue looked swollen and red. I had read somewhere a few years ago that that could be due to a B vitamin deficiency. I take the Seeking Health B-Minus complex every day, which is a formulation from Dr. Ben Lynch that doesn’t have any methylfolate or folic acid in it. (I take the folinic acid separately.) That B-complex has 20 mg of riboflavin in it. The dietary recommendation is something like 1.5 mg per day, so I thought I was getting plenty of riboflavin, but I still had this cracking and redness issue. According to Chris Masterjohn, some people with the MTHFR mutation may need up to 400 mg of riboflavin a day. I started taking 100 mg capsules in addition to my B-complex and guess what?—the redness around my mouth is resolving. I am working my way up to 400 mg a day. Riboflavin is a water-soluble vitamin and any excess is eliminated from the body, so I don’t need to worry about toxicity.
I haven’t solved the entire puzzle yet, but I have way more information than I had 35 years ago. Comprehensive metabolic testing is available, although it’s expensive. I’m going to ask my naturopath about it on my next visit.
I’m not a doctor and I don’t give medical advice. Please don’t ask me. I present this for informational purposes only. If you have questions, ask your doctor.